
If you have a child with dyslexia, there is a very good chance someone you trust has told you some version of this: dyslexia is a lifelong condition. Your child will always have it. The best you can do is help them manage it.
That message comes from pediatricians. From neuropsychologists. From IEP meetings. From Yale’s dyslexia center, from the Cleveland Clinic, from the International Dyslexia Association. It is, in other words, the official consensus. I am going to ask you to hold that consensus lightly for the next few minutes.
Not to dismiss it — the science behind it is real and the people delivering it mean well. But because there is another layer of science — from neuroimaging research conducted over the last two decades — that adds something profound to the picture. Something that most families are never told.
The question “can dyslexia be fixed” deserves a more precise answer than “no,
it’s lifelong.” And the brain science provides one.
WHAT THIS ARTICLE COVERS
- What ‘dyslexia is lifelong’ actually means — and what it doesn’t mean
- What neuroimaging research shows about the dyslexic brain before and after intervention
- The critical distinction between a structural deficit and a functional disconnection
- What neuroplasticity means for your child specifically
- Why the genetics argument doesn’t mean what most parents have been told
- What families who have seen 50 percentile points of improvement actually did differentl
What ‘Dyslexia Is Lifelong’ Actually Means
Let’s start with what the official consensus is actually saying — because it is more nuanced than the way it is usually delivered.
When researchers and clinicians say dyslexia is lifelong, they are making a specific claim: the neurological differences that characterize dyslexia — the differences in how the brain processes written language — do not simply disappear on their own as a child gets older. A child does not outgrow dyslexia the way they outgrow a shoe size. Without targeted intervention, the reading difficulties tend to persist.
That part is true. And it matters, because it means waiting and hoping is not a strategy.
But here is what that statement does not mean — and this is the part that gets lost:
“Lifelong does not mean unchangeable. Those are not the same thing.”
The claim that dyslexia is lifelong is a claim about what happens without adequate intervention. It is not a claim that the underlying neurological profile is fixed and unresponsive to targeted input. And the neuroimaging research — the brain scan evidence — makes this distinction with remarkable clarity.
What Brain Scans Show Before and After Intervention
Over the last two decades, researchers have been able to image the brains of children with dyslexia before and after reading intervention. What they have found has changed the scientific conversation — even if it hasn’t yet changed what most families are told in a pediatrician’s office.
The foundational finding is this: children and adults with dyslexia show a consistent pattern of underactivation and reduced functional connectivity in two specific regions of the left hemisphere. The Parietal-Temporal region — responsible for phonological processing, the mapping of letters to sounds — and the Occipital-Temporal region — responsible for the rapid, automatic recognition of whole word forms.
In a typical reader, these two regions are richly connected and activate efficiently and automatically during reading. In a dyslexic reader, the connection between them is weak or disrupted. The brain’s reading circuitry is not communicating as it should. This is what researchers call a functional disconnection.
Now here is where the pre- and post-intervention imaging becomes important.
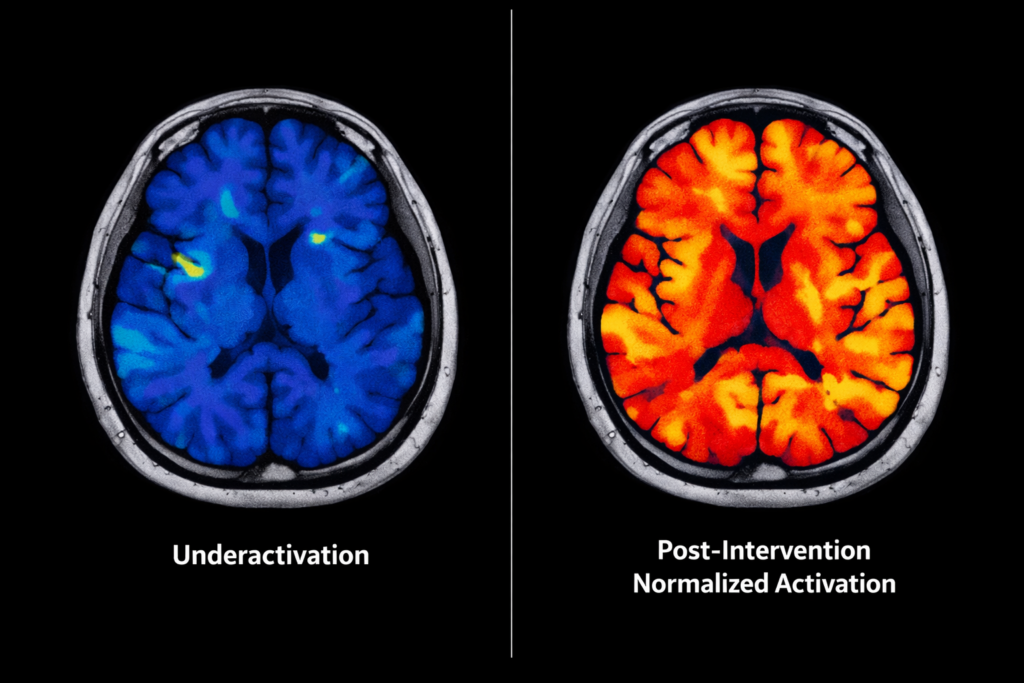
Studies conducted by Dr. Sally Shaywitz and her colleagues at Yale, by Dr. Panagiotis Simos and his team, and by Dr. Guinevere Eden at Georgetown have all demonstrated the same thing: following effective reading intervention, the neuroimaging shows measurable changes in these exact regions. The ParietalTemporal and Occipital-Temporal areas show increased activation. The functional connectivity between them improves. The brain’s reading circuitry begins to operate more like that of a typical reader.
“ The brain changes. Not metaphorically — measurably, on a scan. The functional disconnection that characterizes dyslexia responds to targeted intervention.”
This is not a fringe finding. It is replicated across multiple research groups, using multiple imaging methodologies, in multiple countries. It is, at this point, one of the most robust findings in the neuroscience of reading.
So when someone tells you dyslexia is permanent — they are not describing what the neuroimaging shows. They are describing what happens without effective intervention. The difference is everything.
The Difference Between a Structural Deficit and a Functional Disconnection
This distinction is the one that changes how you think about your child’s future.
A structural deficit is anatomical. Something is physically malformed or absent. Structural deficits are, by definition, far harder to address because you cannot easily change the physical architecture of the brain.
A functional disconnection is different. It is not about the physical structure of the brain — it is about how efficiently two regions are communicating. A functional disconnection means the pathways are present but underactivated. The circuitry exists. It is just not running efficiently.
What the neuroimaging consistently shows in dyslexia is a functional disconnection — not a structural deficit. The Parietal-Temporal and Occipital- Temporal regions are present. The pathways between them exist. What is reduced is the functional connectivity: the efficiency and reliability of the signal transmission between them.
“ Your child’s brain is not missing anything. It has a connection that isn’t running efficiently. And that is a very different clinical picture.”
Functional connectivity responds to targeted stimulation. This is the principle behind physical therapy for stroke rehabilitation, behind cochlear implant training, behind virtually every neurological rehabilitation approach that has demonstrated measurable outcomes. You identify the underactivated pathway. You provide the targeted, repetitive input that drives activation. The brain’s neuroplasticity does the rest.
The same principle applies to the functional disconnection in dyslexia. This is not a theoretical claim. The post-intervention brain scans are the evidence.
Neuroplasticity: What It Actually Means for Your Child
Neuroplasticity is a word that gets used loosely, so let me be precise about what it means in this context.
Neuroplasticity refers to the brain’s capacity to modify its own functional organization in response to experience and input. It is the mechanism by which learning occurs — by which new skills become automatic, by which practicing a musical instrument changes the neural representation of the fingers in the motor cortex, by which a stroke survivor can regain lost function through targeted rehabilitation.
The key principle, first described by the psychologist Donald Hebb and now foundational to neuroscience, is this: neurons that fire together wire together. Repeated, co-activation of neural circuits strengthens the connections between them.
Progressive activation of underactivated pathways — with sufficient frequency and structure — drives myelination, the biological process that speeds and stabilizes neural signal transmission.
This is exactly what effective dyslexia intervention is doing when it works. Not teaching workaround strategies — directly stimulating the underactivated pathways until those pathways strengthen to the point where reading becomes automatic rather than effortful.
The Three Conditions That Drive Neuroplastic Change
Not all intervention drives neuroplastic change equally. The research points to three conditions that distinguish interventions that produce measurable brain changes from those that don’t:
- Targeted specificity — the intervention must activate the specific underconnected pathways, not reading in general
- Daily frequency — the brain consolidates new pathways through consistent daily activation,not infrequent sessions
- Mastery-based progression — each skill must be genuinely consolidated before the next is introduced, ensuring each layer of the neural architecture is stable
When these three conditions are met, the neuroplasticity research is consistent: the brain changes. The functional connectivity improves. Reading becomes more automatic.
When they are not met — when intervention is weekly, unfocused, or paced by time rather than mastery — the results are inconsistent and temporary. This is the neurological explanation for why so many children make progress in intervention and then plateau or regress.
What About the Genetics? If It’s Inherited, Isn’t It Permanent?
This is the question that sits underneath almost every conversation I have with families. And it is the question that most often goes unasked — because parents have been told the answer is yes, and they’ve accepted it.
Dyslexia does have a strong genetic component. The heritability research is well-established. If a parent has dyslexia, their child’s likelihood of having it is significantly elevated. This is not in dispute
But the genetic predisposition and the neurological outcome are not the same thing. This distinction is critical.
“Genetics loads the gun. It does not determine the outcome.”
What the genetic research identifies is a predisposition toward reduced efficiency in the specific cortical networks responsible for reading. What it does not establish is that those networks are unresponsive to targeted intervention. The neuroplasticity research addresses this directly — and the postintervention imaging studies do not exclude individuals based on family history of dyslexia. The brain changes are observed regardless of genetic origin.
Consider the analogy of cardiovascular disease. A strong family history of heart disease creates a genuine, inherited predisposition. But that predisposition does not mean the outcome is fixed — it means the right intervention is more important, not that intervention is pointless. The genetic predisposition sets the starting condition. It does not set the ending one.
Your child inherited a vulnerability in a specific neural pathway. They did not inherit an unchangeable future.
So Can Dyslexia Be Fixed? A Direct Answer
Here is the most honest answer I can give you, grounded in what the neuroimaging research actually shows:
THE DIRECT ANSWER
The functional disconnection that is the neurological basis of dyslexia responds to targeted, neuroplasticity-based intervention.
Post-intervention brain scans demonstrate measurable normalization of PTO activation patterns and improved functional connectivity.
The genetic predisposition does not prevent this response. Whether you call that ‘fixing’ dyslexia is partly a semantic question.
What is not semantic is the outcome: children who complete an effective neuroplasticitybased intervention read more fluently, more automatically, and with significantly less effort than before. Their brains, measurably, function more like typical readers.
Families in the PTO Reconnect Protocol™ average 50 percentile points of reading improvement in 16 weeks. Not through better compensatory strategies — through rebuilding the functional connection that makes reading automatic.
The caveat worth naming honestly: not every child achieves the same outcome. Severity, age at intervention, consistency of practice, and the presence of cooccurring conditions all influence the trajectory. What the research and our clinical outcomes both show is that severity determines pace — it does not determine destination. A child with more severe dyslexia may take longer. They are not beyond reach.
Why This Matters More Than a Semantic Debate
I want to close with something that goes beyond the neuroscience, because I think it matters enormously.
When a parent is told their child has a lifelong condition that must be managed rather than addressed — that message does something. It installs a ceiling on hope.
It shifts the entire frame of the family’s efforts from ‘let’s fix this’ to ‘let’s cope with this.’ And that shift, I have watched over 22 years, changes what parents pursue, what children believe about themselves, and what becomes possible.
The child who is told they will always struggle with reading carries that story. They build their identity around it. They stop trying to read for pleasure. They find ways to hide their difficulty. They internalize the message that their brain is broken.
Their brain is not broken. It has a functional disconnection. And the neuroplasticity research — not optimism, not wishful thinking, but peerreviewed brain scan evidence — shows that functional disconnections can be rebuilt.
“Your child’s brain is not broken. It is disconnected. And we know, from the science, how to rebuild that connection.”
That story — the one where your child’s brain is not defined by its starting condition — is the story the neuroimaging research supports. It is the story I have dedicated my career to telling. And it is the story I believe your child deserves to live.
THE NEXT STEP
If the science in this article raised questions about what effective intervention actually looks like for your child, the next step is to watch our free webinar —Where to Go After the Diagnosis — which walks through the PTO Reconnect Protocol™ in detail: how it works, what families experience, and what the
outcomes data shows.
It is free and it is not a sales presentation. It is the most complete picture of what the neuroplasticity research means in practice for a real child with a real reading profile.
Watch the free webinar at https://retrainthedyslexicbrain.com/landing. And if you want to understand what you can start doing at home right now while you figure out next steps, read How to Help a Dyslexic Child at Home — the practical companion to the science in this article.
About the Author

Dr. Rebecca Troy is an educator, researcher, and learning differences expert
with more than 22 years in classrooms, resource rooms, and IEP meetings. She
holds a doctorate in education, is a Nationally Board Certified Teacher in early
and middle literacy, and is the creator of the PTO Reconnect Protocol™ — a
neuroplasticity-based reading intervention that has helped 3,000+ children
achieve an average of 50 percentile points of reading improvement in 16
weeks. Her work has been featured in Forbes and Psychology Today. She is a
TEDx speaker.




